They deploy
Your data partner runs one script on their infrastructure.
A shared workspace on their hardware, under their control.
You never touch their systems. You never see individual records.
Every collaboration starts with a data access agreement. Every agreement triggers legal, ethics, IT security.
Months pass — or it never happens. tracebloc removes data transfer and direct access — the rest is routine.
How It Works
The problem
The cohort your reviewer wants exists somewhere, but you can't get to it in time. An MTA takes eight months, an Epic integration costs $25k before any line of code is written. The revision deadline is long gone before access can be set up.
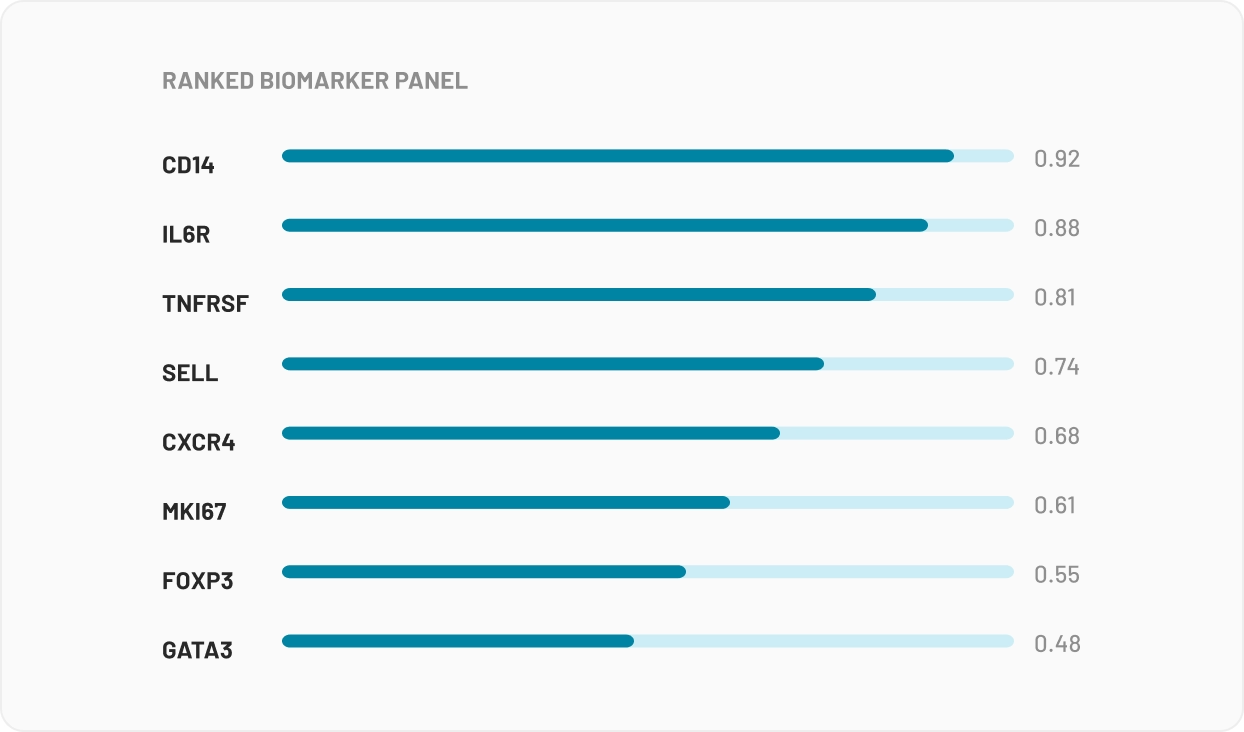
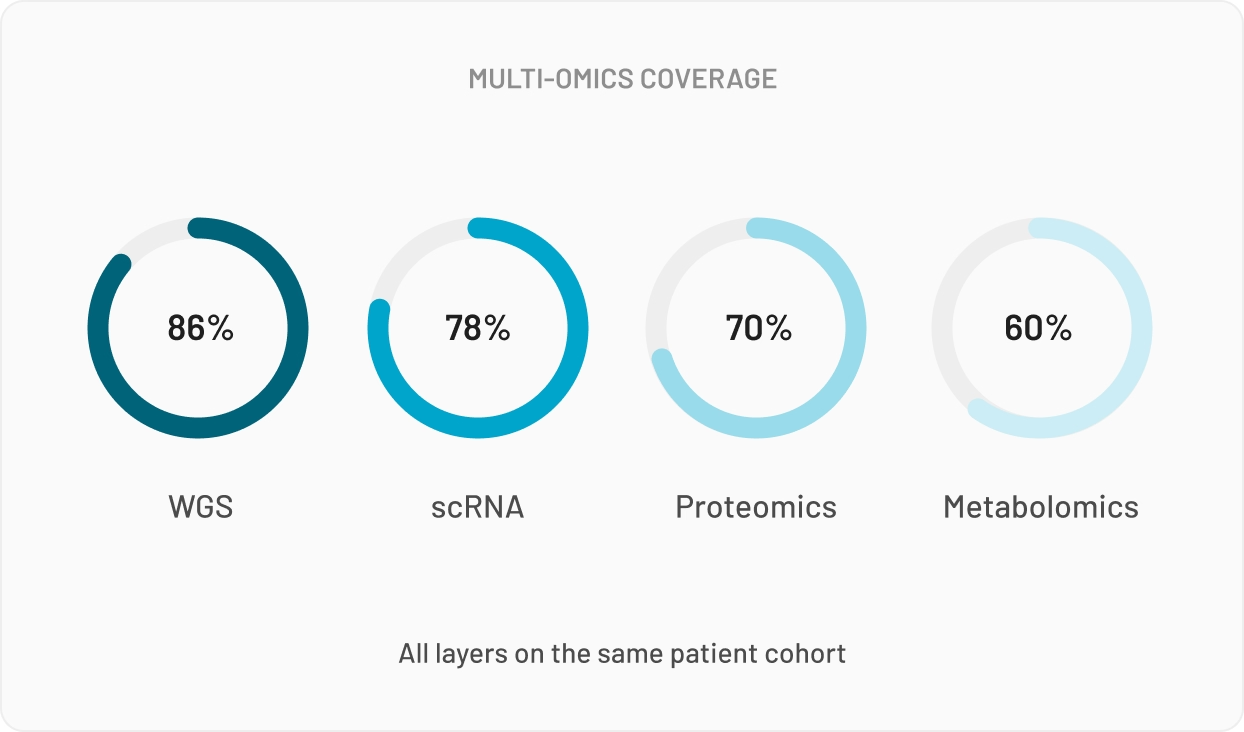
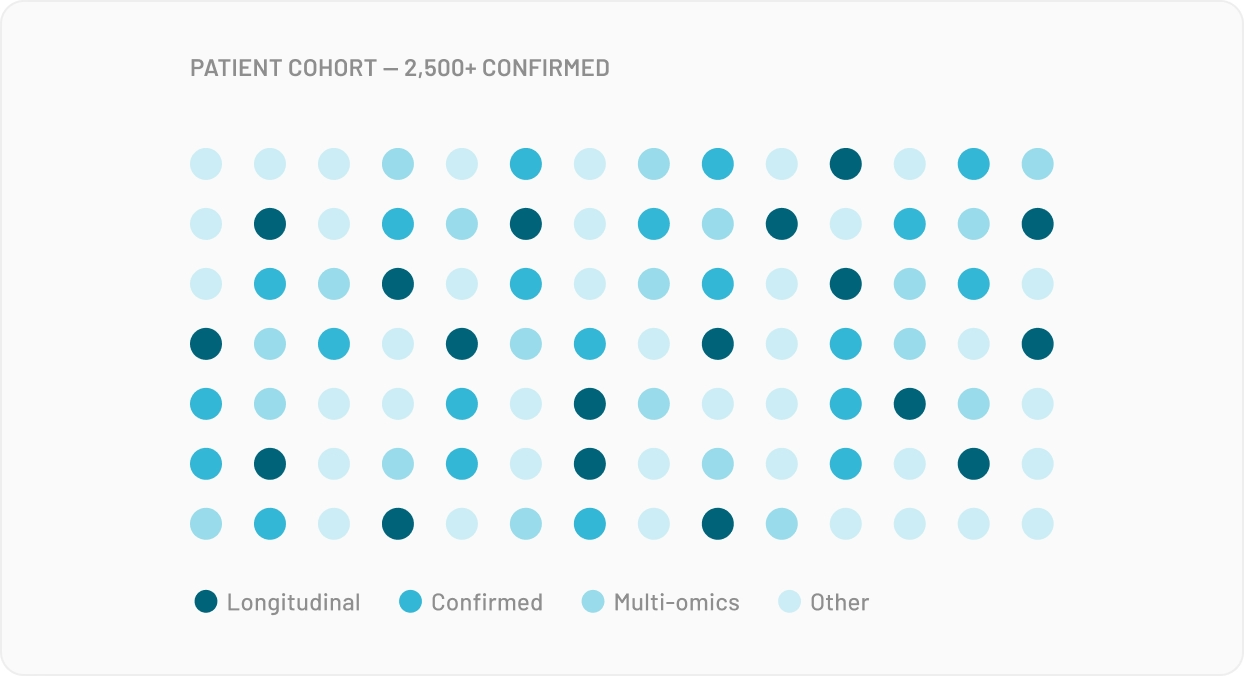
For Multi-Omics data, your n is typically small, and so is everyone else's in your network. Multi-omics needs numbers no single site can produce, which is why bioinformaticians keep asking whether they can combine datasets from different studies. The answer: statistically yes, legally no.
tracebloc is what you give your data partner so they can say yes. They deploy a workspace on their infrastructure. You submit your model. No data leaves their site — so the approval that used to take months is now routine.
The Platform
Use cases
Each scenario maps to how pharma actually acquires and validates clinical data — shaped by conversations with clinical genomics leads, bioinformatics heads, and commercial teams.
WHY Reviewers Trust us
Every model runs in the same container, on the same hardware, with the same seed. No drift between submissions. No "it worked on my machine."
Each run records a hash of the model, data version, and environment. Reviewers can verify the exact run behind every number in your paper.

Validation runs on a partner institution's data — not a held-out slice of your own. The independent cohort your reviewer asks for.

Only results leave the site. Nothing to share, nothing to govern, nothing to unwind if a sample is withdrawn.